Ozempic Arms: The Muscle Loss Pattern Behind the Side-by-Side Photos
"Ozempic arms" became the visible signature of long-term GLP-1 use in 2025–2026 — the muscle wasting that shows up in side-by-side before/after photos and the search trend climbed 120% alongside it. It's not vanity. It's a metabolic warning sign that matters far beyond aesthetics.
The 20–30% of Ozempic weight loss that comes from muscle, not fat — and what it means for your long-term metabolism.
In this guide:
The phrase started as a TikTok observation about celebrities — sudden slimming where the arms looked notably thinner, sometimes hollowed at the triceps. By mid-2025 it had crossed into clinical conversation: endocrinologists started flagging the muscle-loss pattern in their long-term Ozempic patients. By 2026 the search trend caught up — a 120% increase in "ozempic arms" queries as users started recognizing the pattern in their own bodies.
It's easy to dismiss as vanity. It isn't. Muscle is your largest metabolically active tissue — losing significant amounts of it lowers your baseline metabolism, increases rebound risk, and (in users over 50) raises sarcopenia and fall-risk concerns down the road.
What "Ozempic Arms" Actually Means
The honest version, in 40 seconds
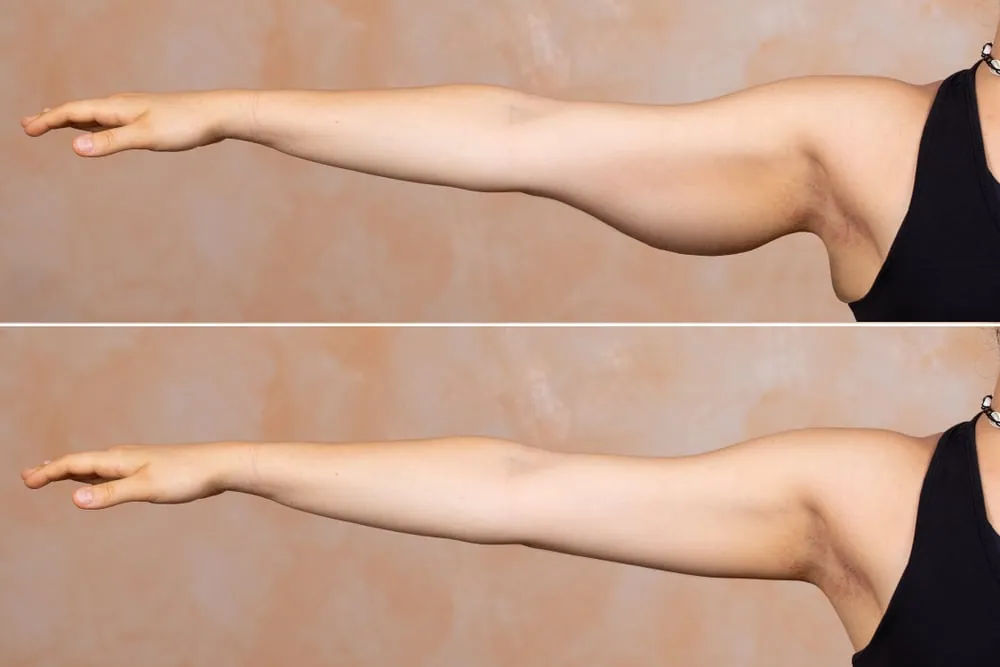
"Ozempic arms" is the visible pattern of muscle loss in the upper arms (triceps + deltoids especially) on long-term GLP-1 users. It reflects a broader issue: 20–30% of total weight loss on GLP-1 drugs comes from lean tissue, not fat. The arms show it first because they have less subcutaneous fat to mask the change. The same loss is happening throughout the body — you just can't see it until it shows up where fat coverage is thinnest.
Clinically, "Ozempic arms" describes:
- Visible thinning of the upper arm — particularly the back of the arm (triceps area) and the shoulder cap (deltoid)
- Loss of muscle tone — the arm looks "deflated" even when relatively lean
- Skin laxity — loose skin where muscle used to fill it out
- Weakness in functional tasks — carrying groceries, opening jars, lifting overhead all feel harder than before
It's the visible piece of a body-wide pattern — same thing happens in legs, back, glutes, but those areas have more fat coverage so the change is masked longer.
Why the Arms Show It First
Three anatomical reasons:
1. Lower subcutaneous fat coverage. Arms naturally carry less fat than the torso, legs, or glutes. When muscle volume decreases, the visual change isn't hidden by overlying fat — it becomes immediately apparent.
2. Smaller muscle groups, faster visible change. Triceps and deltoids are smaller than the large muscles of legs or back. Same percentage loss = more visible difference in smaller muscles.
3. Frequent visual reference. You see your arms in the mirror, in sleeves rolled up, in selfies. You don't watch your thighs or back the same way. The arms get noticed because they're constantly in view.
Why GLP-1 Drugs Cause Muscle Loss
Three mechanisms converge:
1. Suppressed appetite = inadequate protein. Ozempic is so effective at appetite suppression that most users dramatically reduce overall food intake — including protein. Muscle requires daily protein turnover to maintain itself (~0.7–1g per pound of body weight minimum). When intake drops below that threshold, the body breaks down muscle for amino acids. Sustained over months, this produces meaningful lean loss.
2. Rapid weight loss exceeds fat-burning capacity. Healthy fat loss tops out at roughly 1.5–2 lbs per week. Ozempic users routinely lose 3–5 lbs per week, especially in the first months. When weight loss exceeds what your body can sustainably burn as fat, the excess comes from lean tissue. The faster the loss, the higher the muscle percentage.
3. Altered mTOR signaling. The mTOR pathway controls muscle protein synthesis. Emerging research suggests GLP-1 receptor activation may slightly downregulate mTOR signaling in muscle tissue, meaning the body's muscle-building machinery operates at lower capacity even when protein is available. This effect isn't fully characterized yet but appears real.
The Metabolic Cost (It's Worse Than the Aesthetic One)
Lost muscle isn't just about how your arms look. It has direct metabolic consequences:
- Lower baseline metabolism. Muscle burns calories at rest. Less muscle = lower resting metabolic rate. A 10 lb muscle loss can drop your daily calorie burn by 50–80 calories — meaning easier weight regain on the same intake when you eventually stop the drug.
- Higher rebound risk. The combination of reduced metabolism + appetite spike after stopping Ozempic is a primary driver of the 50–70% weight regain that studies document. Muscle loss compounds this dramatically.
- Sarcopenia risk (especially over 50). Age-related muscle loss is already a problem after 50. Adding 10–15 lbs of accelerated loss in a single year can push users into clinical sarcopenia territory — affecting balance, fall risk, bone density, and independence in later decades.
- Reduced insulin sensitivity. Muscle is the primary site of glucose disposal. Less muscle = worse glucose tolerance, which is paradoxical given that GLP-1 drugs are partly prescribed for diabetes.
How to Prevent Ozempic Arms (4-Part Protocol)
Prevention requires deliberate effort throughout your Ozempic course — not a fix you start after noticing the change.
- 1. Protein, aggressively. 1 gram per pound of TARGET body weight daily (not current weight). For a 180-lb person targeting 150 lbs, that's 150g protein daily — divided across 3–4 meals of 30–50g each. Whey protein shakes are often necessary because Ozempic suppresses appetite enough that hitting protein targets through whole food alone is impractical for most users.
- 2. Strength training 2–3x per week. Resistance training is the primary signal that tells your body to preserve muscle during weight loss. Without it, the body has no reason to keep lean tissue when calories are scarce. Focus on compound movements: squats, deadlifts, presses, rows. Progressive overload — slightly heavier or more reps each week — non-negotiable.
- 3. Slow the weight loss rate if possible. Faster loss = more muscle. If you're losing 3+ lbs/week, talk to your doctor about a lower maintenance dose. Slower loss (1–2 lbs/week) preserves dramatically more lean tissue.
- 4. Track and adjust. Monthly DEXA scans or InBody scans can tell you whether you're losing fat or muscle. If lean mass is dropping, that's the signal to add more protein, lift heavier, or slow the loss rate. Without measurement, you only notice the change when it's already visible — too late to fully prevent.
Can You Rebuild What's Lost?
Yes, partially — but it's harder than preventing it. The honest reality:
Muscle rebuilding takes months to years. Even with optimal protein intake and consistent strength training, rebuilding 10–15 lbs of muscle takes 12–24 months for most adults. Older users (50+) rebuild more slowly due to natural anabolic resistance.
You need to STAY off the drug long enough to rebuild. Muscle preservation is harder while still on Ozempic because appetite suppression makes adequate protein intake difficult. Rebuilding typically requires either stopping the drug or transitioning to a much lower maintenance dose.
Some users never fully recover. Particularly those over 50 who took GLP-1s for 18+ months, the muscle loss can be partially permanent. Sarcopenia, once established, is harder to reverse with age.
Bottom line: prevention dramatically outweighs cure here. Catching the loss in the first 1–3 months and addressing it then matters far more than trying to rebuild after a year of cumulative loss.
The Natural Alternative That Preserves Muscle
The honest reality: Ozempic arms is a downstream effect of how dramatically the drug suppresses appetite. Slower, gentler weight loss — the kind natural alternatives produce — doesn't trigger the same muscle-loss cascade because it doesn't crash daily food intake the same way.
Natural GLP-1 supplements work with your body's own appetite signaling rather than overriding it. You eat less than baseline, but not so dramatically less that protein intake collapses. Weight loss is slower (4–8% over 6 months vs Ozempic's 15%) but lean tissue is preserved at much higher rates.
SlimLex GLP-1
Best for natural GLP-1 appetite controlAn Akkermansia + P9 formula that triggers your body's own GLP-1 — for adults who want appetite control without the needle.
- 500+ verified buyers
- 30-day money-back guarantee
Current pricing and bundle options are shown on the official site.
SlimLex GLP-1 supports your body's own GLP-1 production through Akkermansia muciniphila and the P9 protein. Same biological pathway as Ozempic, but the gentler magnitude means appetite doesn't crash to the point where protein intake becomes impossible.
If you'd rather come at the metabolic problem through Berberine and AMPK activation — which has documented effects on insulin sensitivity that complement muscle preservation — the multi-pathway capsule route works:

Ignitra
Best Berberine multi-pathway capsuleBerberine HCL anchor + 10 supporting metabolic ingredients — for adults past 35 dealing with slow metabolism and stubborn cravings.
Check the Latest Price →FAQs
What is Ozempic arms?
'Ozempic arms' is the informal name for visible muscle wasting in the upper arms (especially triceps and deltoid areas) that shows up in long-term Ozempic users. It's part of a broader pattern of lean tissue loss — sometimes called sarcopenia — that affects 20–30% of total weight lost on GLP-1 drugs. The arms tend to show it first because they have less subcutaneous fat coverage than the torso or legs, so muscle loss becomes visible faster.
Why does Ozempic cause muscle loss?
Three reasons. First, Ozempic suppresses appetite so dramatically that most users undereat protein — and muscle requires daily protein turnover to maintain itself. Second, the rapid weight loss rate (3–5 lbs/week common) exceeds what the body can sustainably lose as fat alone, so it cannibalizes lean tissue. Third, GLP-1 drugs slightly alter mTOR signaling (the muscle-building pathway) in ways that aren't yet fully characterized. The combination produces significant lean mass loss across most users.
How much muscle do you lose on Ozempic?
Clinical studies show that 20–30% of total weight loss on GLP-1 drugs comes from lean tissue rather than fat. For someone who loses 50 lbs on Ozempic, that's 10–15 lbs of muscle. Over a full course of treatment, the cumulative muscle loss can be significant enough to lower baseline metabolism, increase sarcopenia risk (especially in users over 50), and create the visible 'Ozempic arms' pattern.
How do I prevent Ozempic arms?
Four interventions matter most. First, eat 1g of protein per pound of target body weight daily — non-negotiable. Second, strength train 2–3x per week with progressive overload, focusing on compound lifts (squats, deadlifts, presses, rows). Third, don't lose weight faster than 1–2 lbs per week if possible — slower loss preserves more muscle. Fourth, if your appetite suppression is too aggressive to hit protein targets, consider asking your doctor about a lower maintenance dose or transitioning to a natural alternative.
Will my arms recover after stopping Ozempic?
Partially, with deliberate effort. Lost muscle can be rebuilt through resistance training + adequate protein, but it takes months to years to fully recover what was lost over a 6–12 month Ozempic course. Older users (50+) recover more slowly than younger users. The honest framing: prevention is dramatically easier than rebuilding. Catching the loss early and addressing it with protein + lifting matters far more than trying to rebuild after the fact.
Final Thoughts
Ozempic arms isn't a vanity issue. It's a metabolic warning that compounds quietly while the scale moves dramatically. 20–30% of the weight you lose on Ozempic is muscle — and that loss lowers your baseline metabolism, raises rebound risk, and (over 50) starts eating into sarcopenia territory that becomes a long-term independence issue.
If you're on Ozempic, start the 4-part prevention protocol now — not after the arms start thinning. If you're considering Ozempic and muscle preservation matters to you, the natural GLP-1 alternative path produces gentler weight loss without the lean-tissue crash. Trade-off is real (lower magnitude) but so is the muscle cost of the pharmaceutical route.
And whatever path you choose: strength train. Eat protein. Track body composition, not just weight. Muscle preservation isn't optional for sustainable weight management — it's the foundation.
Recommended Products
Reviewed by: Michael Anderson, Editor-in-Chief — Last updated:
About Emily Carter
Emily Carter is a contributor at The Supplement Post covering brain and neuro health, blood sugar control, weight loss, gut-focused formulas, and CBD wellness. She specializes in evidence-aware summaries of nootropic ingredients, metabolic supplements, and cannabidiol — with consumer-friendly explanations of how form, dose, and bioavailability shape the result a buyer actually feels.
Emily Carter is not a medical doctor. She analyzes publicly available research to provide evidence-aware summaries for adults exploring cognitive support, metabolic balance, gut wellness, and CBD options.
Disclosure
All content on The Supplement Post is for informational purposes only and is not a substitute for professional medical advice, diagnosis, or treatment. Each product is a dietary supplement, not a prescription drug; statements about its benefits have not been evaluated by the U.S. Food and Drug Administration (FDA) and the product is not intended to diagnose, treat, cure, or prevent any disease.
Results may vary based on individual health status, consistency of use, and lifestyle. If you are pregnant or nursing, taking medication, or have a medical condition, consult a qualified healthcare professional before using any supplement.
This page may contain affiliate links—if you purchase through them, The Supplement Post may earn a small commission at no additional cost to you. References to third-party sites are provided for convenience; we do not control or guarantee their content.